Chapter 8
Chapter 8 of the document provides an in-depth look at education and health services in Rajasthan, focusing on the state’s efforts to promote social development through these crucial sectors. Below is a detailed summary that incorporates factual data, analysis, and objective insights for a clearer understanding of the progress and challenges within these two essential areas.
The development of the social sector is fundamental for achieving sustainable national growth. Investments in education and health are not only beneficial for individual well-being but also contribute significantly to economic productivity and societal welfare. The state government of Rajasthan emphasizes the overall development of all sections of society, particularly focusing on marginalized groups through education and healthcare initiatives.
Objective Insight: The state’s commitment to improving education and health underscores the importance of building human capital, which is critical for long-term economic growth and poverty reduction. Education and healthcare are interdependent; improvements in one sector can significantly enhance outcomes in the other.
- Education in Rajasthan
1.1 Elementary Education: Schools and Enrollment
- Rajasthan operates a substantial number of 29,001 Government Primary Schools (PS), 16,488 Government Upper Primary Schools (UPS), and 19,685 Senior Secondary Schools, ensuring basic education infrastructure throughout the state. The total enrollment in government schools stood at 67.39 lakh in 2022-23.
- Enrollment Data and Teacher-Student Ratio:
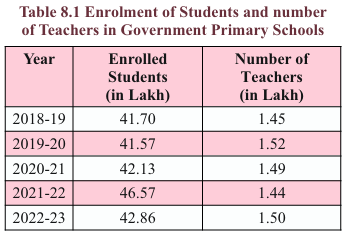
- Enrollment in Primary Schools fluctuated between 41.70 lakh (2018-19) and 42.86 lakh (2022-23), with around 1.50 lakh teachers employed.
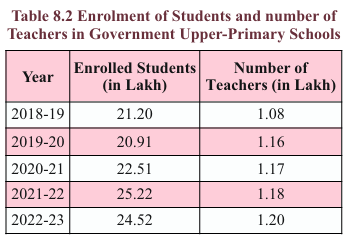
- In Upper Primary Schools, the number of students increased from 21.20 lakh in 2018-19 to 24.52 lakh in 2022-23, with teacher numbers rising to 1.20 lakh in 2022-23.
- Objective Insight: While the state provides a wide network of schools, the teacher-student ratio and quality of education are critical challenges. Teacher availability, particularly in rural areas, needs improvement to ensure equal access to quality education across the state.
1.2 Key Educational Initiatives and Programs
- Free Textbook Distribution Scheme:
- The government distributed 1.99 crore textbooks to students from grades 1 to 8 in the academic year 2023-24. This scheme aims to reduce the financial burden on families and ensure every child has access to learning materials.
- Scholarships and Financial Assistance:
- Pre-metric scholarships worth ₹2,224.10 lakh were distributed to students from SC, ST, OBC, and other disadvantaged groups in 2023-24.
- The Chief Minister Sambal Yojana allocated ₹40 lakh to assist widows and abandoned women pursuing a diploma in elementary education.
- Objective Insight: Programs such as free textbooks and scholarships are essential for improving access to education for disadvantaged groups. However, continuous monitoring is required to ensure that these benefits reach the intended populations and translate into improved learning outcomes.
1.3 Gender-Focused Educational Programs
- Kasturba Gandhi Balika Vidyalayas (KGBVs):
- In 2023-24, Rajasthan operated 316 KGBVs with 41,865 girls enrolled, targeting regions with high educational deprivation for girls. A budget of ₹13,162.02 lakh was allocated for their operations.
- Empowerment Programs for Adolescent Girls:
- Initiatives such as the Kishori Shaikshik Utsav involved over 5.32 lakh girls in educational fairs focused on mathematics and science. Additionally, self-defense training was provided to 27,136 trainers and 20.64 lakh girls.
- Objective Insight: The government’s focus on gender equality in education is essential for empowering girls, particularly in marginalized areas. These programs provide opportunities for continued education and skill development, addressing both gender gaps and social inequities.
1.4 National Education Policy (NEP) 2020 and Samagra Shiksha
- NEP 2020 emphasizes foundational literacy and numeracy and has introduced Bal Vatikas (pre-primary classes) in 1,090 government schools. These initiatives aim to build strong educational foundations for young children.
- Samagra Shiksha: The flagship program targets the universalization of elementary and secondary education. It aims to reduce social and gender gaps in school education, improve learning outcomes, and provide vocational education. The fund-sharing ratio between the central and state government for this scheme is 60:40.
- Objective Insight: By aligning with NEP 2020 and implementing Samagra Shiksha, Rajasthan is taking significant steps toward inclusive and equitable education. However, sustained efforts are required to address challenges such as infrastructure deficits, particularly in remote and rural areas, and ensuring the effective implementation of vocational education.
1.5 Innovations and Support for Marginalized Students
- Inclusive Education for Children with Special Needs (CWSN):
- Rajasthan has prioritized the education of children with special needs by allocating ₹2,918.27 lakh in 2023-24. These funds are used for medical, functional, educational, and therapeutic support, enabling children with disabilities to access quality education.
- The creation of state model resource rooms in Jaipur and Udaipur has further strengthened these efforts, offering specialized services to help CWSN integrate into mainstream education.
- Objective Insight: Providing dedicated support for children with special needs highlights the state’s commitment to inclusive education. However, consistent monitoring and improvements in accessibility, teacher training, and specialized resources are required to ensure that these children can benefit fully from mainstream educational opportunities.
- Higher Education and Vocational Training
2.1 Higher Education in Rajasthan
- Expansion of Colleges and Courses:
- Rajasthan has significantly expanded its higher education network, with 95 new government colleges and 10 new government agricultural colleges established in 2023-24. Additionally, 32 government degree colleges have been upgraded to postgraduate (PG) colleges.
- The state now has 536 government colleges, catering to a wide range of educational disciplines, including law and agricultural education.
- Scholarship Programs:
- Under the Chief Minister Higher Education Scholarship Scheme, ₹3,871.72 lakh was allocated in 2023-24 to support students in government colleges. This initiative aims to reduce financial barriers and increase access to higher education for underprivileged students.
- The Kalibai Bhil Medhavi Chhatra Scooty Yojana benefited meritorious girls from backward classes, with ₹11.24 lakh allocated to provide scooters as incentives for educational performance.
- Objective Insight: Rajasthan’s focus on expanding access to higher education, particularly in rural areas and for underprivileged groups, is a significant step toward promoting equitable access to education. Ensuring that these colleges maintain high-quality standards and provide relevant skill-based education is crucial for enhancing employability among graduates.
2.2 Vocational Education and Training (VET)
- Vocational Schools and Courses:
- As of 2023-24, Rajasthan operates 3,105 vocational education schools, covering 16 sectors. These schools aim to equip students with practical skills relevant to various industries.
- Vocational education has been integrated into both single-sector and double-sector schools, with a total enrolment of 2.81 lakh students.
- Polytechnic Colleges:
- The state also operates 119 polytechnic colleges, offering technical education to over 23,836 students. The government has made significant investments to improve technical education and provide industry-relevant skills to students.
- Objective Insight: Vocational education plays a key role in bridging the gap between education and employment. The state’s focus on expanding vocational schools and polytechnic institutions is a step toward skilling the youth and preparing them for employment in industries that require specific technical skills. However, further collaboration with industry stakeholders is needed to align training with market demands.
- Health Sector in Rajasthan
3.1 Overview of Health Services
- Healthcare Infrastructure:
- As of March 2024, Rajasthan has a vast network of allopathic medical institutions, including 183 hospitals, 813 community health centers, and 15,550 sub-centers.
- A significant expansion in healthcare facilities includes the opening of 519 new sub-centers and upgrading 297 sub-centers to primary health centers (PHCs).
- Objective Insight: While Rajasthan has made substantial progress in expanding its healthcare infrastructure, challenges remain in ensuring equitable access to quality healthcare, especially in rural areas. The expansion of PHCs and sub-centers is a positive step, but ensuring adequate staffing, equipment, and medicines is essential to fully realize the potential of these facilities.
3.2 Key Health Initiatives and Reforms
- Nirogi Rajasthan Abhiyan:
- Launched in 2019, this program aims to provide preventive healthcare for various groups, including the elderly, women, and adolescents. The initiative focuses on managing lifestyle diseases like diabetes, hypertension, and obesity, as well as communicable diseases such as tuberculosis.
- Mukhyamantri Nishulk Nirogi Rajasthan Yojana:
- This scheme provides free access to essential healthcare services, including medicines and diagnostic tests, for all residents of Rajasthan. In 2023-24, 19.71 crore patients received free medicines, with a total expenditure of ₹1,422.13 crore.
- Objective Insight: Rajasthan’s healthcare initiatives demonstrate a strong focus on preventive healthcare and universal health coverage. However, continued investment is needed to improve healthcare delivery in rural and remote areas, where infrastructure and service gaps remain a significant challenge.
3.3 National Health Programs
- National Mental Health Program:
- The state treated 3.02 lakh new patients and conducted 4.67 lakh follow-up sessions under the National Mental Health Program. Additionally, 1,183 mental health camps were organized in 2023-24 to provide widespread access to mental health services.
- National Fluorosis Prevention Program:
- Rajasthan is one of the states most affected by fluorosis, with 4,349 habitations identified as fluoride affected. In 2023-24, 73,748 suspected fluorosis patients were identified, and 24,369 patients received medical treatment under this program.
- Objective Insight: Addressing mental health and fluorosis are critical areas in Rajasthan’s public health strategy. The state’s proactive approach through national programs reflects a growing recognition of the need to tackle both physical and mental health challenges comprehensively. However, improved awareness campaigns and increased outreach are needed to ensure that these services reach the most vulnerable populations.
Conclusion
Chapter 8 provides an in-depth exploration of Rajasthan’s efforts in the education and health sectors, two foundational pillars of socio-economic development. These sectors not only enhance the overall well-being of individuals but also drive long-term economic growth by building human capital. Despite the progress made, challenges remain, especially in ensuring equitable access to quality education and healthcare across the state. Below is an expanded conclusion with key takeaways and final thoughts on Rajasthan’s achievements and areas for future improvement.
- Significant Progress in Education: Expanding Access and Infrastructure
- Rajasthan has successfully expanded its educational infrastructure, establishing a vast network of 29,001 primary schools, 16,488 upper primary schools, and 19,685 senior secondary schools, which together enrolled 67.39 lakh students in 2022-23(ES_RJ_Ch8). Initiatives such as free textbook distribution and scholarship programs for marginalized communities have played a critical role in boosting enrolment and retention rates.
- Key Insight: While Rajasthan has significantly increased access to education, the quality of education—particularly in rural areas—needs further improvement. The state must focus on addressing the teacher-student ratio, improving teacher training, and enhancing learning outcomes to ensure that students are not only enrolled but also receiving a meaningful education.
- Inclusivity and Gender-Focused Initiatives in Education
- Rajasthan has made commendable strides in promoting inclusive education, particularly through programs targeting marginalized groups. Initiatives such as the Kasturba Gandhi Balika Vidyalayas (KGBVs), which enrolled 41,865 girls, and the Meena-Raju Manch program, aimed at empowering girls, have helped improve educational access for girls from backward regions.
- Key Insight: While gender-focused programs have improved girls’ enrollment, challenges such as high dropout rates and gender gaps in higher education remain. Continued efforts to support girl child education, including scholarships, mentorship programs, and community awareness, will be essential to achieving greater gender parity in education.
- Vocational Education and Skill Development: Preparing for Employment
- The state’s emphasis on vocational education and skill development has been a positive step toward addressing the education-employment gap. With 3,105 vocational schools and 119 polytechnic colleges, Rajasthan is working to equip its youth with industry-relevant skills.
- Key Insight: Vocational education offers an opportunity to align skills with market demand, thereby increasing employability among the youth. To further strengthen this sector, industry collaborations, apprenticeship programs, and continuous updates to vocational curricula are required to ensure that the skills being imparted meet the evolving needs of the job market.
- Strengthening Healthcare Infrastructure
- Rajasthan’s healthcare infrastructure has expanded significantly, with 183 hospitals, 813 community health centers (CHCs), and 15,550 sub-centers providing access to medical services across the state. Programs such as the Mukhyamantri Nishulk Nirogi Rajasthan Yojana, which provided free medicines to 19.71 crore patients, have improved access to essential healthcare.
- Key Insight: While the expansion of healthcare facilities has increased access to basic healthcare services, rural healthcare remains a challenge. Ensuring adequate staffing, medical supplies, and infrastructure in rural and remote areas is critical to achieving universal healthcare access in Rajasthan.
- Preventive and Universal Healthcare: Focus on Public Health
- Rajasthan’s focus on preventive healthcare through initiatives such as the Nirogi Rajasthan Abhiyan has been instrumental in addressing non-communicable diseases such as diabetes, hypertension, and tuberculosis. The National Health Programs for mental health and fluorosis prevention have further strengthened public health interventions.
- Key Insight: Preventive healthcare initiatives have contributed to improving health awareness and early diagnosis. However, for these programs to have a lasting impact, the state needs to focus on public health education, screening programs, and infrastructure improvements, especially in underserved communities.
- Addressing Challenges in Health and Education
While Rajasthan has made considerable progress in both education and health, several challenges persist:
- Teacher Shortages and Infrastructure Gaps: In the education sector, teacher shortages, especially in rural schools, remain a significant issue. This is compounded by infrastructure gaps, including the lack of adequate classrooms, learning materials, and technology access.
- Healthcare Accessibility: Although healthcare services have expanded, unequal access remains a major hurdle, particularly in remote regions. There is a pressing need for improved transportation networks, digital health solutions, and telemedicine to bridge this gap.
- Key Insight: Tackling these challenges will require sustained government investment, capacity building, and stronger public-private partnerships to ensure that all residents have access to quality education and comprehensive healthcare services.
Final Thoughts
- Significant progress in expanding access to education and healthcare, especially for marginalized communities.
- Education: Increased enrolment and infrastructure, but challenges remain in teacher shortages, learning outcomes, and gender disparities.
- Vocational education and gender-focused initiatives show promise, but quality of education must be enhanced across the board.
- Healthcare: Expanded primary and community health centers and strong focus on preventive healthcare, yet rural healthcare access needs improvement.
- Key focus areas moving forward: improving quality of services, strengthening rural infrastructure, and ensuring equitable access to both education and healthcare.
- Continued investment in human resources, digital solutions, and public-private partnerships will be crucial for sustained progress and inclusive growth.
In conclusion, while Rajasthan has made impressive strides in expanding access to education and healthcare, it is crucial to focus on quality, equity, and sustainability to ensure that the benefits of these services reach all segments of society. By addressing the challenges of infrastructure, human resource shortages, and regional disparities, Rajasthan can continue on its path toward inclusive social development and improved well-being for all its citizens.
Chapter 8
Table 8.1
Analytical Summary
This table illustrates the trends in student enrollment and teacher availability in government primary schools over a five-year period, from 2018-19 to 2022-23.
- Enrolment Trends:
- Student enrollment remained relatively stable between 2018-19 and 2020-21, hovering around 41-42 lakh students.
- A significant spike in enrollment is observed in 2021-22, where the figure jumps to 46.57 lakh students.
- In the following year (2022-23), enrollment declines slightly to 42.86 lakh, which still represents a noticeable increase compared to earlier years.
- Teacher Availability Trends:
- The number of teachers in government primary schools has remained fairly consistent, ranging between 1.44 lakh and 1.52 lakh during this period.
- There was a slight decrease in the teacher count in 2021-22 (1.44 lakh), coinciding with the year that saw the highest student enrollment.
- In 2022-23, the number of teachers increased to 1.50 lakh, although the student enrollment was lower than the previous year.
Key Data Points
- 2018-19: 41.70 lakh students, 1.45 lakh teachers
- 2021-22: Peak in enrollment with 46.57 lakh students but only 1.44 lakh teachers (lowest teacher count in the period).
- 2022-23: 42.86 lakh students with 1.50 lakh teachers (teacher count rose).
Key Observations
- The highest student-teacher ratio occurred in 2021-22, where enrollment surged to 46.57 lakh students, but the number of teachers dropped to 1.44 lakh. This indicates a potential strain on teaching resources.
- While student enrollment fluctuated, the number of teachers remained relatively stable, with minor adjustments that suggest teacher recruitment was not keeping pace with enrollment variations.
Key Insights
- The increase in enrollment in 2021-22 could have been influenced by various factors such as government policies, population growth, or possibly the migration back to public schooling after the COVID-19 pandemic. The subsequent decline in 2022-23 enrollment may indicate a stabilization of the post-pandemic scenario.
- The marginal rise in teacher numbers in 2022-23 reflects a response to the previous year’s enrollment spike but does not significantly shift the overall student-teacher ratio.
Conclusion
The data reveals an overall consistent but slightly fluctuating enrollment in government primary schools. The stability in teacher numbers highlights the need for closer alignment between teacher recruitment and student intake to prevent future imbalances in the student-teacher ratio. The peak year of 2021-22 demonstrates how sudden increases in student numbers can challenge existing educational resources.
Table 8.2
Analytical Summary
This table presents data on student enrollment and teacher availability in government upper-primary schools over the period from 2018-19 to 2022-23.
- Enrolment Trends:
- Enrollment of students in upper-primary schools started at 21.20 lakh in 2018-19 and saw a slight dip in 2019-20 to 20.91 lakh.
- There was a consistent upward trend from 2020-21 to 2021-22, peaking at 25.22 lakh in 2021-22, indicating growth in the upper-primary level student population.
- The enrollment slightly decreased to 24.52 lakh in 2022-23, but still remained significantly higher than the earlier years.
- Teacher Availability Trends:
- The number of teachers in upper-primary schools shows a steady increase from 1.08 lakh in 2018-19 to 1.20 lakh in 2022-23.
- The teacher count increased gradually each year, indicating a slow but consistent effort to accommodate growing student numbers.
Key Data Points
- 2018-19: 21.20 lakh students, 1.08 lakh teachers
- 2021-22: Peak enrollment of 25.22 lakh students, 1.18 lakh teachers
- 2022-23: 24.52 lakh students with 1.20 lakh teachers, reflecting a balance between teacher recruitment and student intake.
Key Observations
- Unlike the primary school data, the growth in upper-primary student enrollment has been more consistent, with a sharp increase seen from 2020-21 to 2021-22.
- The steady rise in the number of teachers suggests a proportional response to the increase in students, with the teacher-to-student ratio remaining relatively stable over the years.
- The slight decline in student enrollment in 2022-23 could be reflective of demographic shifts or adjustments post-pandemic.
Key Terms
- Upper-Primary Schools: These schools cater to students in grades 6 to 8, typically aged between 11 and 14 years.
- Enrolment: The total number of students registered in upper-primary schools during a specific academic year.
- Teacher-Student Ratio: A metric used to determine the number of teachers available per student, reflecting the capacity of the school system to provide adequate educational resources.
Key Insights
- The increasing number of teachers in upper-primary schools is a positive indicator, suggesting that educational authorities are keeping pace with growing student enrollment, especially during the surge in 2021-22.
- The drop in student numbers in 2022-23, although minimal, may signal a return to pre-pandemic trends or the effect of external factors, such as population aging or migration.
Conclusion
The enrollment trends in government upper-primary schools display a stable upward trajectory from 2018-19 to 2021-22, with teacher numbers consistently increasing. The balance between student numbers and teacher availability appears well-managed, ensuring that the quality of education is maintained through adequate resource allocation. Despite a slight decline in student enrollment in 2022-23, the overall trend points to the effective expansion of educational infrastructure to accommodate the needs of upper-primary students.
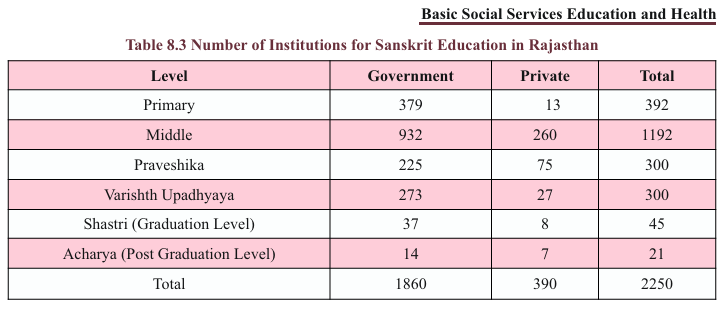
Table8.3
Analytical Summary
This table provides a breakdown of Sanskrit education institutions in Rajasthan, categorized by education levels from primary to post-graduation (Acharya) levels and by whether they are government or private institutions.
- Institution Distribution:
- A total of 2,250 institutions offer Sanskrit education in Rajasthan, with the majority being government-run (1,860 institutions) and a smaller proportion (390) being private institutions.
- The highest concentration of Sanskrit institutions is at the middle level, with 1,192 total institutions (932 government and 260 private).
- Private vs. Government Contribution:
- Government institutions significantly outnumber private ones at almost all levels of Sanskrit education.
- The disparity between government and private institutions is most significant at the middle level, where government institutions account for 78% of the total.
- Private institutions play a larger role at higher education levels (Shastri and Acharya), contributing a noticeable share of institutions, especially at the postgraduate (Acharya) level.
Key Data Points
- Primary: 392 institutions (379 government, 13 private)
- Middle: 1,192 institutions (932 government, 260 private)
- Praveshika: 300 institutions (225 government, 75 private)
- Varishth Upadhyaya: 300 institutions (273 government, 27 private)
- Shastri (Graduation level): 45 institutions (37 government, 8 private)
- Acharya (Post-graduation level): 21 institutions (14 government, 7 private)
Key Observations
- Government institutions dominate Sanskrit education, especially at the primary and middle levels, where private institutions are minimal.
- At higher levels of education (Shastri and Acharya), the presence of private institutions is proportionally greater, suggesting that private institutions focus more on advanced Sanskrit education.
- The number of total institutions progressively decreases from the middle level through to higher education, indicating a narrowing focus or interest as the educational level increases.
Key Terms
- Praveshika: An intermediate level in Sanskrit education, equivalent to secondary education.
- Varishth Upadhyaya: Senior secondary level in Sanskrit education.
- Shastri: Equivalent to a bachelor’s degree in Sanskrit studies.
- Acharya: Equivalent to a master’s degree in Sanskrit studies.
Key Insights
- The dominance of government-run Sanskrit institutions reflects the state’s active role in promoting classical language education.
- The higher proportion of private institutions at the postgraduate level may indicate that private players find greater opportunities or demand in specialized higher-level Sanskrit education.
- Despite the general decline in Sanskrit’s relevance in modern education, Rajasthan maintains a substantial infrastructure for Sanskrit learning, ensuring its continuation at various educational stages.
Conclusion
The distribution of Sanskrit education institutions in Rajasthan highlights a strong governmental role, particularly at foundational levels of education. While private institutions make a smaller contribution, they are more prevalent in advanced Sanskrit education. The overall infrastructure ensures that Sanskrit continues to be a part of Rajasthan’s educational offerings, though interest appears to taper off at the higher education levels.
Table 8.4
Analytical Summary
This table presents data on the number of polytechnic colleges and their total intake capacity in Rajasthan over the last five years, with a distinction between government and private institutions.
- Total Polytechnic Colleges:
- The overall number of polytechnic colleges has decreased consistently over the last five years, from 136 in 2019-20 to 119 in 2023-24.
- The number of government polytechnic colleges remained relatively stable, increasing slightly from 44 in 2019-20 to 49 in subsequent years.
- Private polytechnic colleges, however, saw a steady decline from 92 in 2019-20 to 70 in 2023-24, leading to an overall reduction in total polytechnic institutions.
- Intake Capacity:
- The total intake capacity of polytechnic colleges has reduced over time, with government institutions showing a gradual increase in capacity and private institutions exhibiting a sharp decline.
- Government intake capacity rose from 7,215 in 2019-20 to 8,695 in 2023-24, indicating a focus on expanding access within government institutions.
- Private institution intake capacity dropped significantly from 22,781 in 2019-20 to 15,141 in 2023-24, contributing to the overall decrease in total intake.
Key Data Points
- Total Colleges:
- 2019-20: 136 (44 Govt., 92 Private)
- 2023-24: 119 (49 Govt., 70 Private)
- Intake Capacity:
- 2019-20: 29,996 (7,215 Govt., 22,781 Private)
- 2023-24: 23,836 (8,695 Govt., 15,141 Private)
Key Observations
- The reduction in the number of private polytechnic colleges is a significant trend, while the government sector shows stability and slight growth.
- There is a marked decrease in the total intake capacity of private polytechnic colleges, suggesting declining demand, funding, or regulatory changes affecting private education providers.
- Government institutions, in contrast, have increased their capacity over the same period, which might indicate the government’s focus on offering more technical education opportunities through public institutions.
Key Terms
- Polytechnic Colleges: Institutions that provide technical education, focusing on practical and skills-based learning in engineering and related fields.
- Intake Capacity: The total number of students that can be admitted in a given academic year across all polytechnic institutions.
Key Insights
- The decreasing number of private polytechnic colleges and their intake capacities could reflect challenges faced by private education providers, such as financial difficulties or decreased student interest in private technical education.
- The increase in the number of government polytechnic colleges and their intake capacity suggests a strategic focus by the state government on expanding access to technical education through public institutions.
- The total intake capacity has decreased over the five years, which may imply a declining interest in polytechnic education overall, potentially due to other educational opportunities or market demand shifts in technical fields.
Conclusion
The data highlights a structural shift in the polytechnic education landscape of Rajasthan, with government institutions expanding and private institutions contracting. This trend may reflect broader policy goals or market conditions influencing the demand for and availability of technical education. The decline in total intake capacity suggests a need for further investigation into student preferences and employment trends in polytechnic fields.
Table 8.5
Analytical Summary
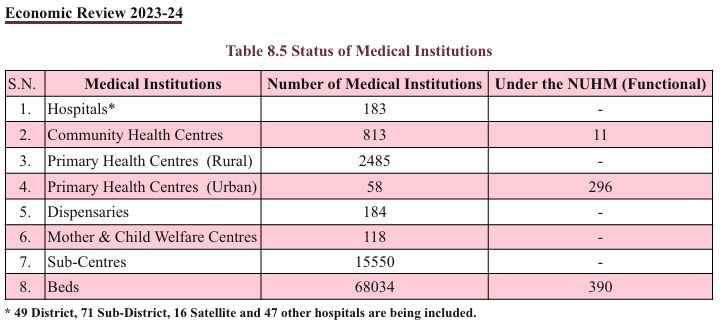
This table provides an overview of the status of medical institutions in Rajasthan, including the number of institutions and their functionality under the National Urban Health Mission (NUHM). The table includes a breakdown of hospitals, community health centres, dispensaries, sub-centres, and available beds.
- Hospitals:
- Rajasthan has a total of 183 hospitals, which includes district, sub-district, satellite, and other hospitals. However, none are listed as functional under the NUHM.
- Community Health Centres (CHCs):
- There are 813 CHCs in the state, of which 11 are operational under the NUHM. CHCs generally provide essential healthcare services, especially in rural and semi-urban areas.
- Primary Health Centres (PHCs):
- The state operates 2,485 rural PHCs and 58 urban PHCs. Notably, 296 of the urban PHCs are functional under the NUHM, reflecting the mission’s focus on improving healthcare access in urban areas.
- Dispensaries:
- There are 184 dispensaries across the state, providing essential medical services but none under the NUHM.
- Mother & Child Welfare Centres:
- Rajasthan operates 118 centres dedicated to maternal and child healthcare, critical for improving healthcare outcomes among vulnerable populations.
- Sub-Centres:
- The state has 15,550 sub-centres, which serve as the most peripheral contact point between the healthcare system and the community, especially in rural areas.
- Beds:
- The total number of available beds in the state stands at 68,034, with 390 functional under the NUHM.
Key Data Points
- Hospitals: 183
- Community Health Centres (CHCs): 813 (11 under NUHM)
- Primary Health Centres (PHCs):
- Rural: 2,485
- Urban: 58 (296 functional under NUHM)
- Sub-Centres: 15,550
- Total Beds: 68,034 (390 under NUHM)
Key Observations
- A large number of healthcare facilities, such as hospitals, CHCs, PHCs, and sub-centres, provide healthcare services across the state, with a significant number concentrated in rural areas.
- Urban healthcare infrastructure is being actively developed under the NUHM, with a significant number of urban PHCs functional under this mission.
- Despite the extensive healthcare network, only a small proportion of institutions, specifically urban PHCs and CHCs, are functional under the NUHM, reflecting a focus on improving urban healthcare.
Key Terms
- NUHM (National Urban Health Mission): A central government initiative to improve healthcare access for urban populations, especially for the poor and marginalized.
- Primary Health Centres (PHCs): Basic healthcare facilities that provide essential healthcare services, typically in rural and semi-urban areas.
- Community Health Centres (CHCs): A higher-level healthcare facility than PHCs, designed to serve a larger population with more specialized services.
- Sub-Centres: Peripheral health units providing the first point of contact for rural populations.
Key Insights
- The majority of healthcare services are still concentrated in rural areas, reflecting Rajasthan’s demographic needs.
- The NUHM is actively functional in urban health centres, specifically focusing on urban PHCs, which indicates an effort to address urban health disparities.
- The large number of sub-centres points to an expansive rural healthcare network, but the lack of NUHM functional sub-centres suggests limited focus on urban-rural healthcare integration under this program.
Conclusion
Rajasthan has a comprehensive network of medical institutions, with a particular focus on rural healthcare infrastructure, including a significant number of PHCs and sub-centres. However, urban areas are seeing increased attention under the NUHM, particularly through the operationalization of urban PHCs. While the overall infrastructure is robust, greater integration of rural institutions into programs like the NUHM could further enhance healthcare access across the state.
Table 8.6

Analytical Summary
This table provides key statistics on the progress of the Mukhaya Mantri Ayushman Arogya Yojana, focusing on the number of treated patients, submitted claims, and paid claims, along with the corresponding financial outlays.
- Treated Patients:
- A total of 3,22,58,887 patients have been treated under the scheme, showcasing the program’s significant reach in terms of healthcare access and provision.
- Claims Submitted:
- A total of 70,04,462 claims have been submitted, with a corresponding monetary value of ₹3,495.90 crore. This indicates the number of claims made by healthcare providers or individuals under the scheme to recover treatment costs.
- Paid Claims:
- Out of the submitted claims, 5,59,18,898 have been approved and paid. The total value of these paid claims stands at ₹2,910.04 crore, representing a high clearance rate of claims.
Key Data Points
- Treated Patients: 3,22,58,887
- Claims Submitted: 70,04,462
- Submitted Claims Value: ₹3,495.90 crore
- Paid Claims: 5,59,18,898
- Paid Claims Value: ₹2,910.04 crore
Key Observations
- The program has treated a large number of patients, providing a substantial contribution to public healthcare.
- The gap between the number of claims submitted and those paid is relatively low, reflecting efficient processing of claims under the scheme.
- The monetary value of paid claims is slightly less than the total submitted claims, indicating some cases where claims may be pending, rejected, or reduced.
Key Terms
- Mukhaya Mantri Ayushman Arogya Yojana: A state healthcare scheme aimed at providing financial protection and access to quality healthcare for economically vulnerable sections of society. It is part of the larger Ayushman Bharat initiative.
- Claims Submitted: Refers to the requests made by hospitals or individuals to the insurance provider for reimbursement of treatment costs.
- Paid Claims: Represents the claims that have been successfully processed and paid by the insurance provider.
Key Insights
- The high number of treated patients demonstrates the scheme’s wide reach and its critical role in the public healthcare system.
- The slight discrepancy between submitted and paid claims suggests there may be pending claims, incomplete documentation, or disputes in claim amounts.
- Financially, the program has disbursed a significant amount, contributing to healthcare costs and reducing the burden on low-income households.
Conclusion
The Mukhaya Mantri Ayushman Arogya Yojana has made substantial progress in providing healthcare services to a large population, with over 3.2 crore patients treated. The efficient processing of claims and disbursal of funds reflect the program’s success in ensuring access to affordable healthcare. However, continued focus on processing pending claims and ensuring the timely release of funds will further strengthen the scheme’s impact.
Table 8.7

Analytical Summary
This table presents the number of various medical institutions related to Ayurveda, Yoga, Naturopathy, and other traditional health systems in the state as of 2023-24. It provides insights into the infrastructure supporting traditional medicine and complementary health practices across the state.
- District Hospitals:
- There are 33 district-level hospitals in the state that cater to Ayurvedic treatments, indicating the regional availability of Ayurvedic healthcare at district levels.
- Ayurvedic Hospitals:
- A total of 90 Ayurvedic hospitals exist, reflecting the state’s commitment to institutionalizing traditional medicine within the public healthcare system.
- Block Ayush Hospitals:
- The state has established 83 Block Ayush hospitals, promoting integrated healthcare that combines Ayurvedic, Yoga, and other traditional systems at the block level.
- Ayurved Dispensaries:
- A large network of 3,579 Ayurvedic dispensaries provides primary healthcare services related to Ayurveda. This indicates significant availability of basic Ayurvedic care across the state.
- Mobile Units:
- There are 14 mobile units providing traditional medicine services, suggesting efforts to reach remote or underserved areas.
- Yoga and Naturopathy Research Centers:
- The state has 33 research centers focused on Yoga and Naturopathy, indicating an academic and scientific approach towards these practices.
- Yoga & Naturopathy Hospitals:
- The state has 3 hospitals dedicated to Yoga and Naturopathy, signifying institutional care within these health modalities.
- Yoga & Naturopathy Dispensaries:
- Similarly, 3 dispensaries are offering primary care services for Yoga and Naturopathy.
Key Data Points
- District Hospitals: 33
- Ayurvedic Hospitals: 90
- Block Ayush Hospitals: 83
- Ayurvedic Dispensaries: 3,579
- Mobile Units: 14
- Yoga & Naturopathy Research Centers: 33
- Yoga & Naturopathy Hospitals: 3
- Yoga & Naturopathy Dispensaries: 3
Key Observations
- The state demonstrates a comprehensive infrastructure for traditional medicine, particularly Ayurveda, with a strong network of hospitals and dispensaries.
- The large number of Ayurvedic dispensaries (3,579) indicates significant availability of Ayurvedic care at the grassroots level.
- Mobile units and specialized institutions such as Yoga and Naturopathy Research Centers emphasize the state’s focus on promoting wellness and preventive healthcare through traditional practices.
- The smaller number of Yoga and Naturopathy hospitals and dispensaries suggests that these are still emerging fields compared to the more established Ayurvedic care network.
Key Terms
- Ayurvedic Dispensaries: Primary healthcare centers focused on providing Ayurvedic treatments.
- Ayush Hospitals: Integrated healthcare facilities offering services in Ayurveda, Yoga, Naturopathy, Unani, Siddha, and Homeopathy.
- Yoga and Naturopathy: Holistic health systems emphasizing physical well-being, mental discipline, and natural healing.
Key Insights
- The extensive network of Ayurvedic institutions reflects Rajasthan’s emphasis on traditional and alternative medicine in its public healthcare strategy.
- The presence of mobile units and research centers underlines a dynamic approach towards spreading awareness and conducting scientific inquiry into traditional health systems.
- Yoga and Naturopathy, though not as prevalent as Ayurveda in terms of infrastructure, are receiving growing attention, as seen in the establishment of specialized hospitals and research centers.
Conclusion
Rajasthan has developed a robust infrastructure for traditional healthcare, with particular emphasis on Ayurveda. While there is room for further development in Yoga and Naturopathy, the state’s commitment to integrating traditional health systems into its overall healthcare framework is evident. This holistic approach is likely to benefit rural areas and promote preventive care practices.
Table 8.8
Analytical Summary
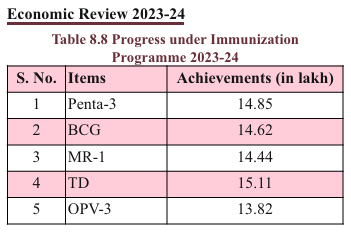
This table highlights the achievements of Rajasthan’s immunization program for the year 2023-24. It shows the number of immunizations administered for different vaccines, measured in lakhs (100,000 units).
- Penta-3 (Pentavalent Vaccine):
- 14.85 lakh doses of Penta-3 were administered. This vaccine protects against five diseases: Diphtheria, Pertussis, Tetanus, Hepatitis B, and Haemophilus influenzae type B (Hib).
- BCG (Bacillus Calmette-Guérin):
- 14.62 lakh doses of BCG were administered. BCG is primarily used to protect against tuberculosis (TB), especially in children.
- MR-1 (Measles-Rubella Vaccine, first dose):
- 14.44 lakh doses of the first measles-rubella vaccine were administered. MR vaccine is critical in preventing both measles and rubella, which can cause severe complications in children.
- TD (Tetanus-Diphtheria Vaccine):
- 15.11 lakh doses of TD were administered, indicating a strong emphasis on preventing tetanus and diphtheria among children and pregnant women.
- OPV-3 (Oral Polio Vaccine, third dose):
- 13.82 lakh doses of OPV-3 were administered as part of the ongoing effort to eradicate polio.
Key Data Points
- Penta-3: 14.85 lakh doses
- BCG: 14.62 lakh doses
- MR-1: 14.44 lakh doses
- TD: 15.11 lakh doses
- OPV-3: 13.82 lakh doses
Key Observations
- The administration of over 14 lakh doses of each major vaccine indicates that the state is maintaining a high level of immunization coverage.
- The highest number of doses administered was for TD (15.11 lakh), which is essential for preventing infections such as tetanus, especially among pregnant women and young children.
- OPV-3, essential for polio eradication, recorded the lowest coverage among the vaccines, though still significant at nearly 14 lakh doses.
Key Terms
- Penta-3: A combination vaccine that offers protection against five potentially life-threatening diseases (Diphtheria, Pertussis, Tetanus, Hepatitis B, and Hib).
- BCG: A vaccine primarily used against tuberculosis, commonly given to children in countries with high TB prevalence.
- MR-1: The first dose of the Measles-Rubella vaccine, vital for preventing measles and rubella.
- TD: A vaccine providing protection against tetanus and diphtheria.
- OPV-3: The third dose of the Oral Polio Vaccine, crucial for polio prevention.
Key Insights
- The immunization program in Rajasthan shows strong coverage for all major vaccines, reflecting a well-functioning public health system in this regard.
- The high number of TD vaccines administered (15.11 lakh) suggests a targeted focus on preventing tetanus and diphtheria, diseases with higher risks in underserved and rural areas.
- The relatively lower figure for OPV-3, while still significant, indicates the need for ongoing attention to polio eradication efforts.
Conclusion
Rajasthan’s immunization program for 2023-24 has demonstrated a robust achievement across multiple vaccines, ensuring widespread coverage and protection against critical diseases. The data reflects a well-implemented public health initiative focused on preventing childhood illnesses, maintaining the state’s progress toward achieving broader immunization targets. Further focus on OPV-3 will be necessary to ensure the continued eradication of polio.
Table 8.9
Analytical Summary
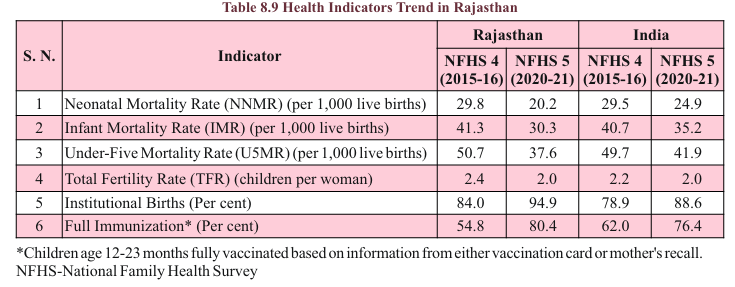
This table compares key health indicators in Rajasthan and India as a whole between two rounds of the National Family Health Survey (NFHS 4: 2015-16 and NFHS 5: 2020-21). It provides insights into maternal and child health improvements, institutional births, fertility rates, and immunization coverage over time.
Key Data Points (Rajasthan)
- Neonatal Mortality Rate (NNMR):
- NFHS 4 (2015-16): 29.8 deaths per 1,000 live births
- NFHS 5 (2020-21): 20.2 deaths per 1,000 live births (significant reduction)
- Infant Mortality Rate (IMR):
- NFHS 4 (2015-16): 41.3 deaths per 1,000 live births
- NFHS 5 (2020-21): 30.3 deaths per 1,000 live births (substantial improvement)
- Under-Five Mortality Rate (U5MR):
- NFHS 4 (2015-16): 50.7 deaths per 1,000 live births
- NFHS 5 (2020-21): 37.6 deaths per 1,000 live births
- Total Fertility Rate (TFR):
- NFHS 4 (2015-16): 2.4 children per woman
- NFHS 5 (2020-21): 2.0 children per woman (reduction)
- Institutional Births (Percentage):
- NFHS 4 (2015-16): 84.0%
- NFHS 5 (2020-21): 94.9% (notable increase)
- Full Immunization (Percentage):
- NFHS 4 (2015-16): 54.8% of children fully immunized
- NFHS 5 (2020-21): 80.4% (significant progress)
Key Observations
- Neonatal Mortality Rate (NNMR), Infant Mortality Rate (IMR), and Under-Five Mortality Rate (U5MR) have significantly decreased, reflecting better maternal and child healthcare, improved medical infrastructure, and vaccination coverage.
- The Total Fertility Rate (TFR) shows a decline from 2.4 to 2.0, which aligns with trends of declining family sizes due to increasing awareness of family planning.
- There has been a 10.9% increase in institutional births, which is crucial for reducing maternal and infant mortality.
- Full immunization coverage has shown remarkable improvement, rising from 54.8% to 80.4%, indicating progress in the state’s public health campaigns.
Key Terms
- Neonatal Mortality Rate (NNMR): The number of deaths of infants aged 0-28 days per 1,000 live births.
- Infant Mortality Rate (IMR): The number of deaths of infants under one year old per 1,000 live births.
- Under-Five Mortality Rate (U5MR): The probability of a child dying before reaching five years of age, per 1,000 live births.
- Total Fertility Rate (TFR): The average number of children a woman would have in her lifetime.
- Institutional Births: Percentage of deliveries that occur in healthcare institutions (hospitals, clinics).
- Full Immunization: The percentage of children aged 12-23 months who have received all the basic vaccinations, including BCG, OPV, DPT, and measles vaccines.
Key Insights
- The improvements in NNMR, IMR, and U5MR are strong indicators of Rajasthan’s enhanced healthcare systems, particularly in maternal and child health services.
- The reduction in TFR signifies improved access to family planning services and the state’s efforts to manage population growth.
- The rise in institutional births and immunization rates reflects government policies promoting safer childbirth and better early childhood care.
Conclusion
Rajasthan has made substantial progress in several critical health indicators from 2015-16 to 2020-21, as reflected in reduced mortality rates, increased institutional births, and higher immunization coverage. These improvements align with national trends and indicate strong governmental intervention and community health initiatives that are positively affecting health outcomes for women and children. However, there remains scope for further progress, especially in neonatal and child mortality rates, which, while improved, are still significant.
Table 8.10
Analytical Summary
This table highlights the Maternal Mortality Rate (MMR) trend for Rajasthan and India between two time periods: SRS (2017-19) and SRS (2018-20). MMR is a crucial health indicator representing the number of maternal deaths per lakh (100,000) live births, reflecting the risk associated with pregnancy and childbirth.
Key Data Points
- Rajasthan:
- SRS (2017-19): 141 maternal deaths per lakh live births
- SRS (2018-20): 113 maternal deaths per lakh live births (significant reduction)
- India:
- SRS (2017-19): 103 maternal deaths per lakh live births
- SRS (2018-20): 97 maternal deaths per lakh live births (overall improvement)
Key Observations
- Reduction in MMR:
- Rajasthan has shown a significant reduction in maternal deaths, improving from 141 in 2017-19 to 113 in 2018-20.
- While Rajasthan’s MMR is still higher than the national average, the 28-point improvement signifies progress in maternal health services, including better access to institutional deliveries and antenatal care.
- National Comparison:
- The MMR for India improved from 103 to 97, a more modest reduction compared to Rajasthan.
- Rajasthan’s MMR is still above the national average, indicating a need for continued focus on maternal health interventions within the state.
Conclusion
The trend shows a positive trajectory in maternal health for both Rajasthan and India. The reduction in MMR reflects improvements in healthcare infrastructure, emergency obstetric care, and better prenatal and postnatal services. However, with Rajasthan’s MMR still higher than the national average, further policy efforts are needed to bring the state’s maternal health indicators closer to the national benchmarks. This includes increasing institutional births, addressing rural healthcare gaps, and improving access to quality maternal health services.
Table 8.11

Analytical Summary
This table presents projected demographic indicators for Rajasthan between 2011 and 2035. It includes vital health and population metrics such as population growth rate, crude birth and death rates, infant mortality, total fertility rate, and life expectancy for males and females. The projections offer insights into the long-term demographic transitions in the state.
Key Data Points
- Population Growth Rate:
- Projected to decline from 16.0% in 2011-15 to 7.6% in 2031-35, indicating slowing population growth.
- Crude Birth Rate (CBR):
- Expected to decrease significantly from 24.3 in 2011-15 to 14.9 by 2031-35, reflecting a reduction in birth rates over time.
- Crude Death Rate (CDR):
- Slight reduction from 7.8 in 2011-15 to 6.8 by 2031-35.
- Infant Mortality Rate (IMR):
- Shows a gradual improvement from 53 in 2011-15 to 36 by 2031-35, indicating better neonatal and maternal healthcare.
- Under-5 Mortality Rate (q5):
- Decreases from 73 in 2011-15 to 50 by 2031-35, showing improvements in child health and survival.
- Total Fertility Rate (TFR):
- Declines steadily from 2.95 in 2011-15 to 1.87 in 2031-35, indicating movement toward lower fertility and population stabilization.
- Life Expectancy:
- Males: Life expectancy is projected to increase from 65.7 years in 2011-15 to 70.7 years by 2031-35.
- Females: Life expectancy is projected to increase from 70.4 years in 2011-15 to 74.8 years by 2031-35.
Key Observations
- Slower Population Growth: The decreasing population growth rate suggests Rajasthan is transitioning to a more stabilized population structure by 2035, with significantly lower fertility rates.
- Improved Health Outcomes:
- The decline in both the Infant Mortality Rate (IMR) and Under-5 Mortality Rate (q5) reflects improvements in maternal and child healthcare services, immunization, and access to healthcare.
- Fertility Transition:
- The significant decline in Total Fertility Rate (TFR) shows the state is moving toward replacement-level fertility, with families having fewer children over time.
- Life Expectancy Gains:
- The gradual increase in life expectancy for both males and females suggests improvements in healthcare infrastructure and lifestyle, with females consistently having a higher life expectancy than males.
Conclusion
The demographic projections for Rajasthan from 2011 to 2035 reflect significant transitions toward lower birth rates, improved child health outcomes, and longer life expectancy. These trends align with national efforts to improve healthcare, promote family planning, and increase access to education, especially for women. As Rajasthan continues to improve its health indicators, it is likely to witness more sustainable population growth, higher life expectancy, and a demographic shift toward an aging population.